Hospitals want supplies ready at the moment of care without extra steps for staff. Touchless hospital inventory management delivers that outcome by pairing vision with automation. Rooms record shelf changes as they happen, orders trigger on signal, and leaders get a reliable view of what is on hand. The goal is a steady shift from reactive counts to continuous control.
How touchless hospital inventory management works
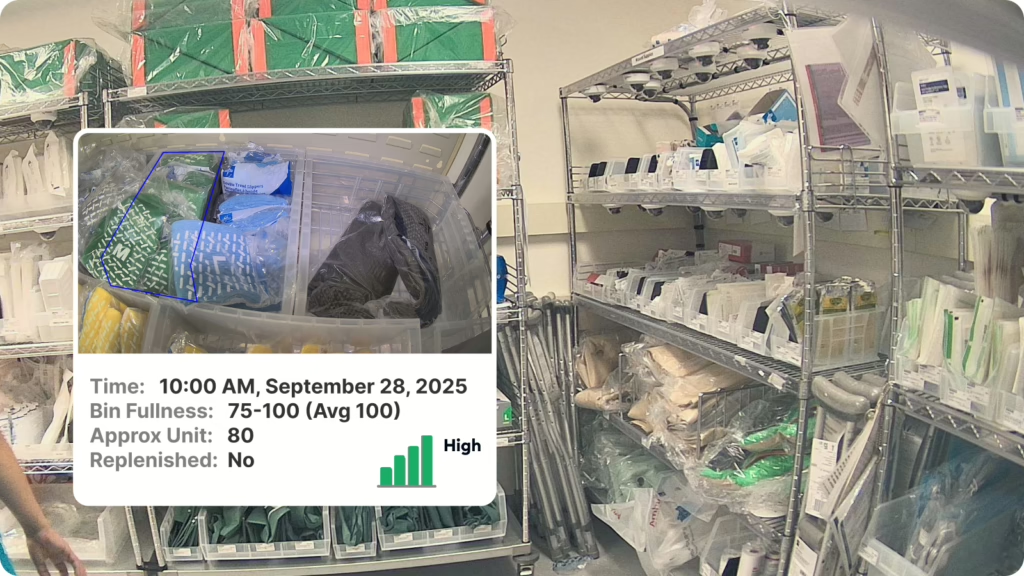
In a zero-touch model, the room becomes the system of record. Smart cameras observe shelves and bins, convert images into SKU events, and post time-stamped levels to a control tower. With computer vision ai, the system identifies products, packaging forms, and quantities, then ties each position to a location map. The result is hands-free stock tracking that functions across open racks, carts, and cabinets.
Since images are the source of truth, teams do not rely on taps or scans to log usage. This no-scan inventory pattern captures change at the shelf and keeps the record current. Signals flow to the ERP or MMIS to issue demand when a bin crosses its threshold. Results across visibility, accuracy, and replenishment appear in five ways AI is transforming healthcare inventory management.

From image signals to accurate orders
Signals from each bin are evaluated against targets that match clinical use. The control tower calculates risk, ranks exceptions, and forms purchase requests for the ERP. Computer vision ai pairs each image with a shelf map and SKU catalog, so counts remain stable even when packaging sizes vary. As usage shifts, par automation adjusts targets so replenishment matches demand without overfill.
Order creation occurs without a person scanning or submitting a ticket. The moment a bin dips below its threshold, the system forms a clean demand file, posts it to purchasing, and captures an audit trail. This keeps the no-scan inventory record synchronized with real movement and prevents drift that creeps in when teams update spreadsheets after a rush. Legacy scans miss shelf changes that cameras capture, and the gaps and advantages are clear in barcode and RFID versus computer vision in hospital supply rooms.
KPIs leadership watches and proof points
Leaders track a tight set of metrics to confirm value.
- Stockouts, by closet and by item, to confirm availability at the point of use.
- On-hand inventory days, to reduce working capital while protecting service levels.
- Replenishment latency, to monitor signal-to-fulfillment time.
- Cycle-count variance, to verify accuracy.
- Clinical time spent on supply tasks, to return time to care.
Programs see measurable shifts in the first quarter when rooms are mapped and targets are tuned. Internal benchmarks show sustained reductions in stockouts once thresholds stabilize, lower working capital as overfill is removed, and sharp declines in manual counting as orders form from signal. Weekly exceptions lists surface items that trend low or high so leaders can right-size targets and address root causes with materials, nursing, and sourcing. Hands-free stock tracking gives teams the data to tune, then hold gains.
Deployment signals that matter
Programs that scale share common markers. Teams stabilize two units per week after the first month. Stockouts drop sharply once thresholds settle, with many units sustaining reductions above 90%. On-hand inventory falls in the 20% to 30% range when governance is active. Manual counting shrinks as ordering shifts from keystrokes to events. Ranges depend on mix, supplier performance, and cadence of review.
Governance and security that sustain trust
Privacy comes first in supply rooms. Systems mask faces, suppress frames with people, and store inventory metadata only. The platform does not collect PHI, patient records, or staff identifiers. Security is standard-based. Traffic uses TLS 1.2 or higher. Deploy on-prem, in the cloud, or hybrid. Role-based access governs who can change mappings and thresholds.
Hospitals require auditability. Each event records location, SKU, level, confidence, and timestamp. Change logs capture who modified shelf maps or targets. Retention follows policy aligned to NIST and the HIPAA Security Rule. Models are validated against your packaging and layouts, monitored for drift, and exceptions receive human review.
These controls keep programs within hospital security posture while enabling touchless hospital inventory management at scale.
Security posture at a glance
- Face masking and people-frame suppression: faces are blurred by default and frames with people present can be suppressed to reduce exposure.
- Metadata only, no PHI: the system stores SKU, bin, location, timestamp, quantity, and confidence. Images do not persist unless explicitly whitelisted for model quality review.
- TLS 1.2+ encryption: all traffic is encrypted in transit with modern ciphers, and mutual TLS can be enabled where required.
- Role-based access control: least-privilege roles govern mapping edits, threshold changes, and administration. MFA is supported.
- Event-level audit trail: immutable logs capture user, action, before and after values, timestamp, and source system.
- Policy-aligned retention: retention schedules follow hospital policy with configurable lifetimes and secure deletion procedures.
- Model validation and drift monitoring: models are validated on your packaging and layouts before go-live, then monitored for accuracy with alerts on drift for review.
Zero-touch Inventory Defined
- PAR level: Target on-hand quantity between replenishments. Why it matters: Signals adjust PAR from real use, which cuts overfill.
- Safety stock: Buffer inventory that absorbs variability. Why it matters: Dynamic buffers shrink as variability drops, which reduces excess.
- Stockout: Required item not available at time of need. Why it matters: Continuous shelf sensing flags risk early, which triggers timely replenishment.
- Cycle count: Periodic spot check to verify records. Why it matters: Staff shift from counting to reviewing exceptions, which saves time.
- Inventory Control Tower: Central dashboard for status, alerts, and trends. Why it matters: Prioritizes high-impact exceptions, which speeds ordering.
- Point-of-Use (POU): Storage near the care setting. Why it matters: Sensing at POU ties demand to actual care, which improves accuracy.
- Real-time reordering: Automatic trigger when a bin crosses its threshold. Why it matters: Removes lag from manual entry, which stabilizes supply.
- Vision AI: Enables smart cameras to turn video into structured inventory events. Why it matters: It identifies barcodes, estimates bin fullness, and posts location and time for touchless tracking.
Measured results for availability, waste, and staff time
Zero-touch narrows the gap between consumption and record. Rooms refill at the right time, emergency orders decline, and waste falls as replenishment better matches use. Unit managers see fewer hunt-and-find moments, which shortens room turns and smooths schedules. Finance gains reliable charge capture and cleaner spend visibility by closet and category. Network leaders can compare service levels across sites and act on exceptions instead of averages.
These gains compound with scale. As more closets and SKUs enter the same loop, forecasting improves, suppliers deliver on plan, and teams spend less time counting and searching. Many programs reach ROI in under a year through reduced overstock, lower labor on supply tasks, and fewer urgent purchases. The shift reflects how AI moves hospital inventory management from stockouts to strategy.
Next steps for leaders
Set success in clear terms, then expand deliberately. Choose a unit with variable demand and engaged clinical leadership. Establish baselines for stockouts, on-hand levels, emergency orders, and staff time on supply tasks. Map the closet, confirm item-to-slot accuracy, and enable par automation with governance from clinical leaders. Hold weekly reviews to adjust targets, resolve chronic exceptions, and confirm that demand files post cleanly to the ERP. The goal is a durable, hospital-wide model of touchless hospital inventory management.
If you want shelves that restock themselves and leaders who can act on reliable data, request a consultation to review your rooms, targets, and KPIs.